Recovering from ACL surgery? Praxis Physiotherapy delivers structured, evidence-based ACL rehab to help you return to life, sport, and everyday function. Learn more.

Recovering from ACL surgery? Praxis Physiotherapy delivers structured, evidence-based ACL rehab to help you return to life, sport, and everyday function. Learn more.

Discover why hamstring strains are so common in running athletes, including personal insights from elite-level sports physiotherapy. This article explores hamstring injury causes, early symptoms, prevention strategies like Nordic hamstring exercises, and the best rehabilitation practices to recover stronger and reduce reinjury risk.

Cricket Side Strains in Fast Bowlers: Causes, Prevention, and Rehabilitation Cricket, a sport demanding significant physical prowess—especially from fast bowlers—often sees athletes pushing their bodies to the limit. This intensity, while integral to performance, can...

The age old question: What's the best gym activity for my sport? Well - the answer should always be "it depends". Even the same athlete playing the same sport will have different requirements at different parts of a season. Generally speaking, there are some common...

We often get asked what are the benefits of one form of exercise versus another. Sometimes this is as simple as discussing the difference between cardio and weights. Today's article focuses on the difference between a two types of gym based loading programs Bilateral...

Summary: Restriction of blood flow purportedly creates an internal environment of greater stress, thus greater adaptation Importantly, the greater adaptation can occur with less absolute load to damaged or painful tissues Started in healthy population to build muscles...

Menopause alters hormones and results in physical changes These changes typically result in increased injury risk or activity reduction The most common injuries affect structures such as the plantar fascia, tendons of the hip and shoulder Appropriate exercise and...
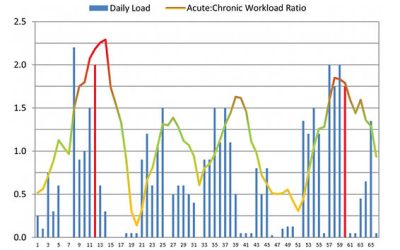
ANSWER: FICTION (Mostly - stay with us here) 🙊 Do you keep getting injured when you get back into your usual training after a period of rest 😤? The first graph shows a 65-day cycle of an Olympic athlete. The red lines indicate when the athlete was injured. Looking at...

Answer: FICTION 🙊 Progressive strength training in the elderly (>60 years) is efficient, even with higher intensities, to improve bone health, pack on muscle and retain function. And not surprisingly, side effects are rare! Strength training increases muscle strength...

Do you have a 'good' and 'bad' shoulder? Have you been putting up with that grumbly shoulder for weeks, months or even years? Shoulder pain can but a real dampener on your activity levels - but it doesn't need to! We at Praxis, pride ourselves on taking the time to...

Answer - FACT With preseason training just around the corner, this blog is a timely reminder that turning up to preseason training consistently will give athletes the best chance of being able to play most games next year. Murray et al (2017) reported that AFL players...

GROIN PAIN Groin pain, referred to also as athletic pubalgia, is a common problem for a number of athletes, particularly those who engage in sports that require specific use (or overuse) of lower abdominal muscles and the proximal muscles of the thigh. Predominantly,...

We at Praxis think that patient education is the cornerstone of good physiotherapy. We particularly enjoy discussing people's understanding of their injuries or the beliefs around certain activities. As such we are starting "Fact or Fiction Friday's" in which we...

For those of you who have ever read a research article and thought it was a tough read, i'd like to let you in on a little secret. Doing the research is far worse! If only memes were a thing when I started my Masters of Applied Science thesis, I'd have changed my...