Struggling with tennis elbow that won’t settle? Discover why recovery takes time and whether cortisone or PRP is the right option for long-term results.

Struggling with tennis elbow that won’t settle? Discover why recovery takes time and whether cortisone or PRP is the right option for long-term results.
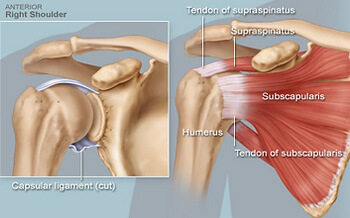
Rotator cuff repair is a common surgery for persistent shoulder pain and dysfunction, but the real progress happens during rehabilitation. This blog outlines what to expect from physiotherapy in each recovery phase—from sling use and pain control to strength and return to sport—backed by the latest research and expert clinical practice at Praxis Physiotherapy.

Discover how starting physiotherapy up to six weeks before your knee replacement surgery can significantly improve your recovery. At Praxis Physiotherapy, our expert-led programs integrate reformer Pilates, blood flow restriction training, and access to on-site gyms to support your rehabilitation every step of the way. Whether you’re referred by Dr. Kelly Macgroarty or another orthopaedic specialist, we’re here to help you move with confidence.

Neck pain is one of the most common – and frustrating – conditions we treat at Praxis Physiotherapy. Whether it’s from poor posture, long desk hours, or simply no clear cause at all, persistent neck pain can have a big impact on your daily life. In this blog, we break down what causes non-specific neck pain, why targeted strengthening and manual therapy are backed by research, and how physiotherapy can help you move, feel, and function better.

We are all guilty of it. Putting off seeing someone about that niggle. "it will be right" we tell ourselves as we trudge on through life, sport and recreation. The "wait and see" approach, when applied to acute musculoskeletal injuries, refers to a common tendency for...
Knee Osteoarthritis is a common ailment responsible for pain, loss of function and reduced quality of life Rates of knee OA are set to increase Whilst there is no cure, exercise therapy under the guidance of a physiotherapist is considered a front line treatment to...

I need to get an MRI to help with the management of my lower back pain Answer - FICTION In a recent narrative review, Wang and colleagues (2018) concluded that MRI imaging in the early stages of lower back pain can have detrimental effects including more pain, less...

Do you have a good knee and a bad knee? Do your knees snap, crackle and pop? Do you ever wish you could walk for longer without pain or not be worried about how your knees will feel in the morning if you were living your life to the fullest? Knee pain is a very common...

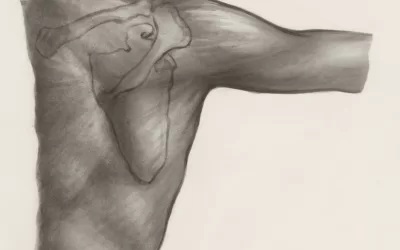
Answer: FICTION. The devil is in the detail! The rotator cuff is a group of 4 muscles that aid in providing stability through range for the shoulder joint, particularly overhead. There are multiple risk factors for RC tears, but most are down to overactivity of the...
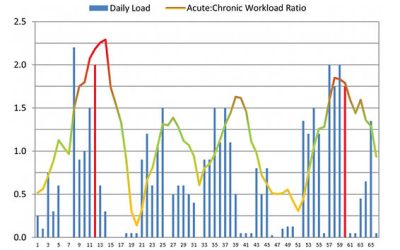
ANSWER: FICTION (Mostly - stay with us here) 🙊 Do you keep getting injured when you get back into your usual training after a period of rest 😤? The first graph shows a 65-day cycle of an Olympic athlete. The red lines indicate when the athlete was injured. Looking at...
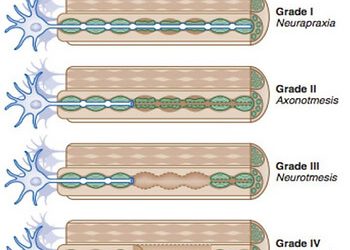
SUMMARY: Stingers are essentially a tractioning of the neural system This can cause pain, movement and sensation changes Chronic traction to the nervous system can have a cumulative effect on nerve function The more damage to the nerve, the more serious the outcome We...

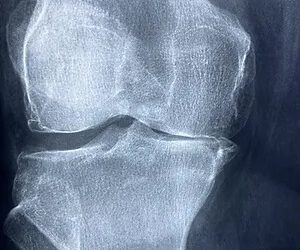
Answer: FICTION 🙊 “Osteoarthritis” is a common term that gets used by our patients as an explanation of their knee pain. But is this always the case 🤔? 🔍In a recent systematic review estimates of osteoarthritis feature prevalence on MRI among asymptomatic uninjured...

Do you have a 'good' and 'bad' shoulder? Have you been putting up with that grumbly shoulder for weeks, months or even years? Shoulder pain can but a real dampener on your activity levels - but it doesn't need to! We at Praxis, pride ourselves on taking the time to...

Sharp catch of pain? Ongoing aches? Trouble getting out of bed or with long car rides? Stiff and sore when you are bending over to pick things up? Referred pain into you legs? If you've experienced any of these symptoms recently you are not alone. Lower back pain is a...

Are you a weekend warrior who is plagued by injury or an aspiring athlete trying to find that extra 1% or somewhere in between? We know how frustrating it can sitting on the side lines and not being able to be involved in the things that make you happy. All the Praxis...

GROIN PAIN Groin pain, referred to also as athletic pubalgia, is a common problem for a number of athletes, particularly those who engage in sports that require specific use (or overuse) of lower abdominal muscles and the proximal muscles of the thigh. Predominantly,...

PODCAST Something a little different for Praxis Physio recently with our principal physio Stephen, having a chat with Matt from Back Yourself fitness. The latest episode is all about rehab, recovery, Praxis Pilates and physio assessments. Some interesting stories...
That age old question in which the answers seems to be becoming increasingly more difficult to answer. We have looked over the research and tried to simply things for those who are unsure about what to do with their shoulder. SUMMARY: A rotator cuff (RC) tear is a...

FICTION! Stay with me on this one as it can be confusing. Pain = An unpleasant sensory and emotional experience associated with actual or potential tissue damage. The best way to sum it up is the above photo. This unlucky gent stuck a nail through his shoe. He was in...

We at Praxis think that patient education is the cornerstone of good physiotherapy. We particularly enjoy discussing people's understanding of their injuries or the beliefs around certain activities. As such we are starting "Fact or Fiction Friday's" in which we...

With our 30 day pilates challenge starting today, we thought we would take a look at why we love pilates so much for our patients, and what some of the benefits are. Part 1 looks at how pilates affect those with chronic lower back pain. Part 2 looks at the difference...
Running. Probably one of the most maligned exercises when it comes to knees and overuse injuries. The thought that running 'wears' out your knees and causes osteoarthritis (a chronic disease often associated with joint pain and stiffness, reduced mobility and reduced...