Struggling with tennis elbow that won’t settle? Discover why recovery takes time and whether cortisone or PRP is the right option for long-term results.

Struggling with tennis elbow that won’t settle? Discover why recovery takes time and whether cortisone or PRP is the right option for long-term results.

ACL reconstruction is just the beginning. At Praxis Physiotherapy in Brisbane, our expert-led, week-by-week rehab plan takes you from prehab to full return-to-sport. Learn how our proven approach, trusted by elite Brisbane teams and surgeons, helps you recover stronger and smarter.

Struggling with shoulder pain that’s holding you back? Learn how athletes can overcome rotator cuff injuries without surgery through expert physiotherapy, targeted rehab, and a sport-specific return plan.
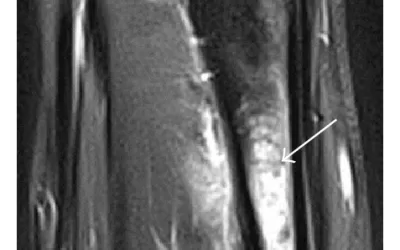
Stress fractures are one of the most common — and frustrating — injuries in runners. This blog explores how these injuries develop, who’s most at risk, and what the latest research says about effective rehabilitation and prevention. Learn how strength and conditioning, smart training loads, and early diagnosis can help you return to running stronger than ever.
Recovering from a shoulder stabilisation surgery, particularly a Bankart repair, can feel like navigating a winding trail. At Praxis Physiotherapy, we understand that athletes don’t just want to heal – they want to return stronger, more confident, and ready for...

If you play a jumping sport like volleyball, basketball or AFL and feel a nagging pain at the front of your knee when you jump, land or change direction, you may be developing patellar tendinopathy. This article explains why it happens, who’s most at risk, and how physio-led rehab helps you get back to full power.
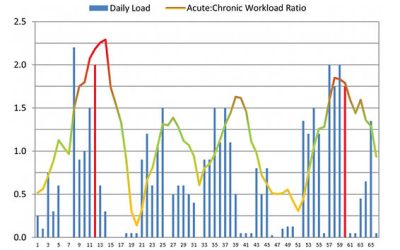
ANSWER: FICTION (Mostly - stay with us here) 🙊 Do you keep getting injured when you get back into your usual training after a period of rest 😤? The first graph shows a 65-day cycle of an Olympic athlete. The red lines indicate when the athlete was injured. Looking at...
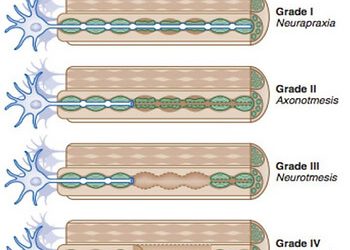
SUMMARY: Stingers are essentially a tractioning of the neural system This can cause pain, movement and sensation changes Chronic traction to the nervous system can have a cumulative effect on nerve function The more damage to the nerve, the more serious the outcome We...

Do you have a “good” shoulder and a “bad” shoulder? Have you been putting up with that grumbly shoulder for weeks, months or even years? Shoulder pain can put a real dampener on your activity levels — but it doesn’t need to....

Are you a weekend warrior who is plagued by injury or an aspiring athlete trying to find that extra 1% or somewhere in between? We know how frustrating it can sitting on the side lines and not being able to be involved in the things that make you happy. All the Praxis...

Key Takeaways Shin splints (MTSS) are an overuse bone stress injury. Training load errors are the biggest contributor. Hip strength and force control play a major role. Early management prevents stress fractures. Strength + smart loading beats rest alone. Shin Splints...

Answer - FACT With preseason training just around the corner, this blog is a timely reminder that turning up to preseason training consistently will give athletes the best chance of being able to play most games next year. The EvidenceMurray et al (2017) reported that...

GROIN PAIN Groin pain, referred to also as athletic pubalgia, is a common problem for a number of athletes, particularly those who engage in sports that require specific use (or overuse) of lower abdominal muscles and the proximal muscles of the thigh. Predominantly,...

THROWING This week in professional development session, our physio team delved into throwing techniques and links to injury. Proper throwing mechanics are important to understand as they may enable an athlete to achieve maximum performance with minimum chance of...

Running. Probably one of the most maligned exercises when it comes to knees and overuse injuries. The thought that running 'wears' out your knees and causes osteoarthritis (a chronic disease often associated with joint pain and stiffness, reduced mobility and reduced...